http://www.youtube.com/watch?v=kXmaMEdtmiE&feature=related
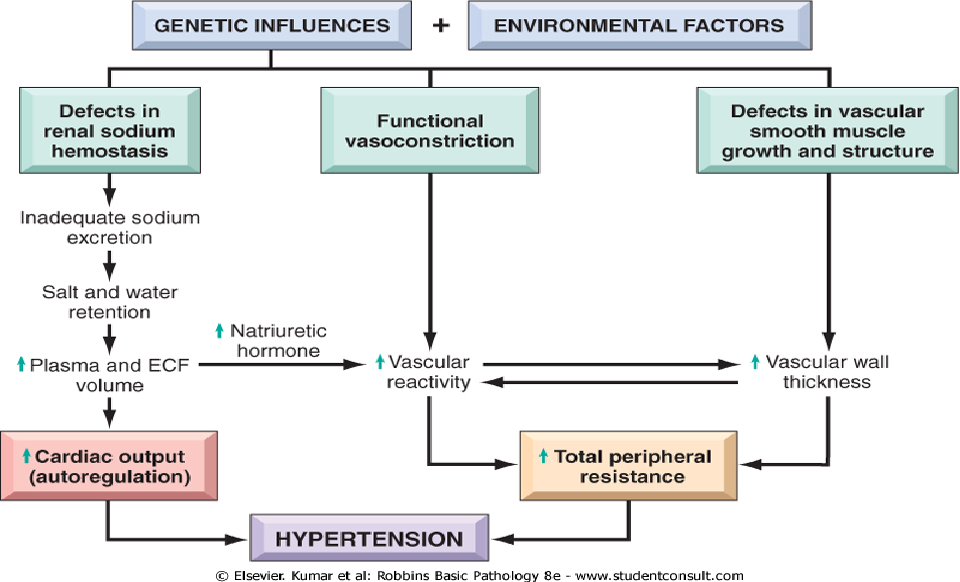
Pathophysiology The pathogenesis of essential hypertension is multifactorial and highly complex. Multiple factors modulate the blood pressure (BP) for adequate tissue perfusion and include humoral mediators, vascular reactivity, circulating blood volume, vascular caliber, blood viscosity, cardiac output, blood vessel elasticity, and neural stimulation. A possible pathogenesis of essential hypertension has been proposed in which multiple factors, including genetic predisposition, excess dietary salt intake, and adrenergic tone, may interact to produce hypertension. Although genetics appears to contribute to essential hypertension, the exact mechanism has not been established.
The natural history of essential hypertension evolves from occasional to established hypertension. After a long invariable asymptomatic period, persistent hypertension develops into complicated hypertension, in which end-organ damage to the aorta and small arteries, heart, kidneys, retina, and central nervous system is evident.
The progression of essential hypertension is as follows:
Cortisol reactivity, an index of hypothalamic-pituitary-adrenal function, may be another mechanism by which psychosocial stress is associated with future hypertension. In a prospective substudy of the Whitehall II cohort, with 3 years follow-up of an occupational cohort in previously healthy patients, investigators reported 15.9% of the patient sample developed hypertension in response to laboratory-induced mental stressors and found an association between cortisol stress reactivity and incident hypertension.
The natural history of essential hypertension evolves from occasional to established hypertension. After a long invariable asymptomatic period, persistent hypertension develops into complicated hypertension, in which end-organ damage to the aorta and small arteries, heart, kidneys, retina, and central nervous system is evident.
The progression of essential hypertension is as follows:
- Prehypertension in persons aged 10-30 years (by increased cardiac output)
- Early hypertension in persons aged 20-40 years (in which increased peripheral resistance is prominent)
- Established hypertension in persons aged 30-50 years
- Complicated hypertension in persons aged 40-60 years
Cortisol reactivity, an index of hypothalamic-pituitary-adrenal function, may be another mechanism by which psychosocial stress is associated with future hypertension. In a prospective substudy of the Whitehall II cohort, with 3 years follow-up of an occupational cohort in previously healthy patients, investigators reported 15.9% of the patient sample developed hypertension in response to laboratory-induced mental stressors and found an association between cortisol stress reactivity and incident hypertension.