Most people with high blood pressure have no signs or symptoms, even if blood pressure readings reach dangerously high levels.
Although a few people with early-stage high blood pressure may have dull headaches, dizzy spells or a few more nosebleeds than normal, these signs and symptoms typically don't occur until high blood pressure has reached a severe — even life-threatening — stage.
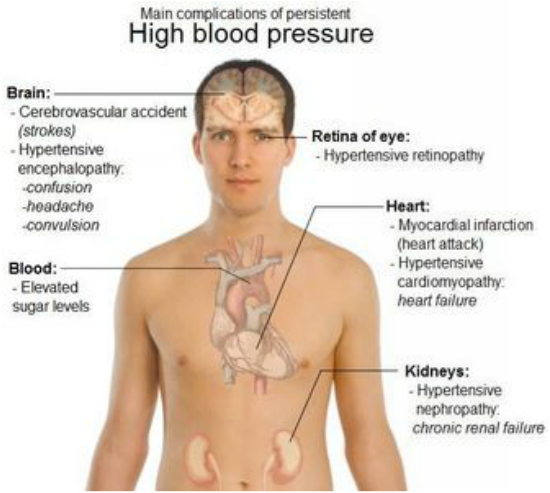
The clinical and laboratory findings are mainly referable to involvement of the target organs: heart, brain, kidneys, eyes, and peripheral arteries.
SYMPTOMS
Mild to moderate primary (essential) hypertension is largely asymptomatic for many years. The most frequent symptom, headache, is also very nonspecific. Suboccipital pulsating headaches, occurring early in the morning and subsiding during the day, are said to be characteristic, but any type of headache may occur. Accelerated hypertension is associated with somnolence, confusion, visual disturbances, and nausea and vomiting (hypertensive encephalopathy).
Hypertension in patients with pheochromocytomas that secrete predominantly norepinephrine is usually sustained but may be episodic. The typical attack lasts from minutes to hours and is associated with headache, anxiety, palpitation, profuse perspiration, pallor, tremor, and nausea and vomiting. Blood pressure is markedly elevated, and angina or acute pulmonary edema may occur. In primary aldosteronism, patients may have muscular weakness, polyuria, and nocturia due to hypokalemia; malignant hypertension is rare. Chronic hypertension often leads to left ventricular hypertrophy, which may be associated with diastolic or, in late stages, systolic dysfunction. Exertional and paroxysmal nocturnal dyspnea may result, and ischemic heart disease is more common (especially when concomitant coronary artery disease is present).
Cerebral involvement causes:
(1) stroke due to thrombosis or
(2) small or large hemorrhage from microaneurysms of small penetrating intracranial arteries.
Hypertensive encephalopathy is probably caused by acute capillary congestion and exudation with cerebral edema. The findings are usually reversible if adequate treatment is given promptly. There is no strict correlation of diastolic blood pressure with hypertensive encephalopathy; but it usually exceeds 130 mm Hg.
SIGNS
Like symptoms, physical findings depend on the cause of hypertension, its duration and severity, and the degree of effect on target organs.
1.Blood pressure- On initial examination, pressure is taken in both arms and, if lower extremity pulses are diminished or delayed, in the legs to exclude coarctation of the aorta. An orthostatic drop is present in pheochromocytoma. Older patients may have falsely elevated readings by sphygmomanometry because of noncompressible vessels. This may be suspected in the presence of Osler's sign - a palpable brachial or radial artery when the cuff is inflated above systolic pressure. Occasionally, it may be necessary to make direct measurements of intra-arterial pressure, especially in patients with apparent severe hypertension who do not tolerate therapy.
2.Retinas- Narrowing of arterial diameter to less than 50% of venous diameter, copper or silver wire appearance, exudates, hemorrhages, or papilledema are associated with a worse prognosis.
3.Heart and arteries- Left ventricular enlargement with a left ventricular heave indicates severe or long-standing hypertrophy. Older patients frequently have systolic ejection murmurs resulting from calcific aortic sclerosis, and these may evolve to significant aortic stenosis in some individuals. Aortic insufficiency may be auscultated in up to 5% of patients, and hemodynamically insignificant aortic insufficiency can be detected by Doppler echocardiography in 10-20%. A presystolic (S4) gallop due to decreased compliance of the left ventricle is quite common in patients with sinus rhythm.
4.Pulses- The timing of upper and lower extremity pulses should be compared to exclude coarctation of the aorta. All major peripheral pulses should be evaluated to exclude aortic dissection and peripheral atherosclerosis, which may be associated with renal artery involvement.
Like symptoms, physical findings depend on the cause of hypertension, its duration and severity, and the degree of effect on target organs.
1.Blood pressure- On initial examination, pressure is taken in both arms and, if lower extremity pulses are diminished or delayed, in the legs to exclude coarctation of the aorta. An orthostatic drop is present in pheochromocytoma. Older patients may have falsely elevated readings by sphygmomanometry because of noncompressible vessels. This may be suspected in the presence of Osler's sign - a palpable brachial or radial artery when the cuff is inflated above systolic pressure. Occasionally, it may be necessary to make direct measurements of intra-arterial pressure, especially in patients with apparent severe hypertension who do not tolerate therapy.
2.Retinas- Narrowing of arterial diameter to less than 50% of venous diameter, copper or silver wire appearance, exudates, hemorrhages, or papilledema are associated with a worse prognosis.
3.Heart and arteries- Left ventricular enlargement with a left ventricular heave indicates severe or long-standing hypertrophy. Older patients frequently have systolic ejection murmurs resulting from calcific aortic sclerosis, and these may evolve to significant aortic stenosis in some individuals. Aortic insufficiency may be auscultated in up to 5% of patients, and hemodynamically insignificant aortic insufficiency can be detected by Doppler echocardiography in 10-20%. A presystolic (S4) gallop due to decreased compliance of the left ventricle is quite common in patients with sinus rhythm.
4.Pulses- The timing of upper and lower extremity pulses should be compared to exclude coarctation of the aorta. All major peripheral pulses should be evaluated to exclude aortic dissection and peripheral atherosclerosis, which may be associated with renal artery involvement.
DEFINITIONS OF MEDICAL TERMS USED ABOVE:
Aortic Dissection: An aortic dissection is a serious condition in which a tear develops in the inner layer of the aorta, the large blood vessel branching off the heart. Blood surges through this tear into the middle layer of the aorta, causing the inner and middle layers to separate (dissect). If the blood-filled channel ruptures through the outside aortic wall, aortic dissection is often fatal.
Aortic Sclerosis: Aortic valve thickening (sclerosis) without stenosis is common in elderly adults [1]. It is often detected either as a systolic murmur on physical examination or on echocardiography performed for some other reason. Aortic valve sclerosis is important clinically because it can progress to aortic stenosis and is a marker for increased cardiovascular risks,
Aortic Stenosis: Aortic valve stenosis — or aortic stenosis — occurs when the heart's aortic valve narrows. This narrowing prevents the valve from opening fully, which obstructs blood flow from your heart into your aorta and onward to the rest of your body.
Murmurs: A heart murmur is an extra or unusual sound heard during a heartbeat. Murmurs range from very faint to very loud. Sometimes they sound like a whooshing or swishing noise. Normal heartbeats make a "lub-DUPP" or "lub-DUB" sound. This is the sound of the heart valves closing as blood moves through the heart. Doctors can hear these sounds and heart murmurs using a stethoscope.
Osler's sign: An indication of acute bacterial endocarditis in which smallcircumscribed painful erythematous swellings appear in the skinand the subcutaneous tissues of the hands and feet.
Papilledema: Papilledema is an optic disc swelling that is secondary to elevated intracranial pressure. In contrast to other causes of optic disc swelling, vision usually is well preserved with acute papilledema. Papilledema almost always presents as a bilateral phenomenon and may develop over hours to weeks.
Peripheral Atherosclerosis: The term peripheral vascular disease is commonly used to refer to peripheral artery disease (PAD), meaning narrowing or occlusion by atherosclerotic plaques of arteries outside of the heart and brain.
Pheochromocytomas: A pheochromocytoma (fe-o-kro-mo-si-TOE-muh) is a rare, usually noncancerous (benign) tumor that develops in the core of an adrenal gland. You have two adrenal glands, one just above each of your kidneys. Your adrenal glands produce hormones that give instructions to virtually every organ and tissue in your body.
Aortic Dissection: An aortic dissection is a serious condition in which a tear develops in the inner layer of the aorta, the large blood vessel branching off the heart. Blood surges through this tear into the middle layer of the aorta, causing the inner and middle layers to separate (dissect). If the blood-filled channel ruptures through the outside aortic wall, aortic dissection is often fatal.
Aortic Sclerosis: Aortic valve thickening (sclerosis) without stenosis is common in elderly adults [1]. It is often detected either as a systolic murmur on physical examination or on echocardiography performed for some other reason. Aortic valve sclerosis is important clinically because it can progress to aortic stenosis and is a marker for increased cardiovascular risks,
Aortic Stenosis: Aortic valve stenosis — or aortic stenosis — occurs when the heart's aortic valve narrows. This narrowing prevents the valve from opening fully, which obstructs blood flow from your heart into your aorta and onward to the rest of your body.
Murmurs: A heart murmur is an extra or unusual sound heard during a heartbeat. Murmurs range from very faint to very loud. Sometimes they sound like a whooshing or swishing noise. Normal heartbeats make a "lub-DUPP" or "lub-DUB" sound. This is the sound of the heart valves closing as blood moves through the heart. Doctors can hear these sounds and heart murmurs using a stethoscope.
Osler's sign: An indication of acute bacterial endocarditis in which smallcircumscribed painful erythematous swellings appear in the skinand the subcutaneous tissues of the hands and feet.
Papilledema: Papilledema is an optic disc swelling that is secondary to elevated intracranial pressure. In contrast to other causes of optic disc swelling, vision usually is well preserved with acute papilledema. Papilledema almost always presents as a bilateral phenomenon and may develop over hours to weeks.
Peripheral Atherosclerosis: The term peripheral vascular disease is commonly used to refer to peripheral artery disease (PAD), meaning narrowing or occlusion by atherosclerotic plaques of arteries outside of the heart and brain.
Pheochromocytomas: A pheochromocytoma (fe-o-kro-mo-si-TOE-muh) is a rare, usually noncancerous (benign) tumor that develops in the core of an adrenal gland. You have two adrenal glands, one just above each of your kidneys. Your adrenal glands produce hormones that give instructions to virtually every organ and tissue in your body.
